
Hepatic Vascular Disease
Mindy M. Horrow, MD, FACR
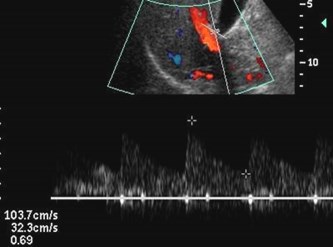
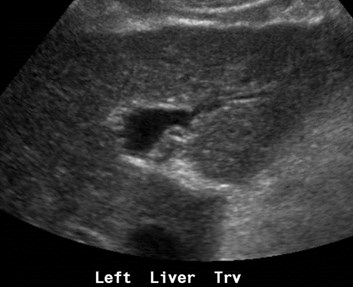
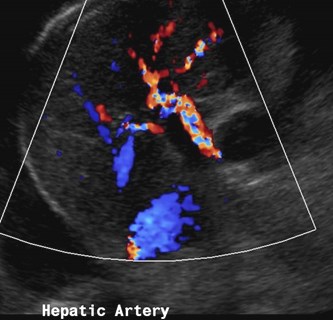
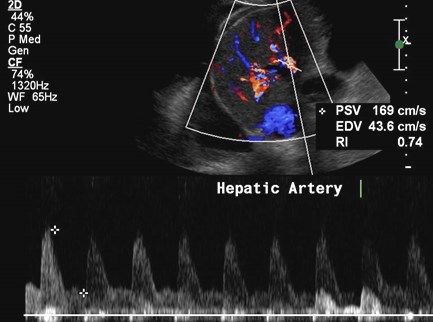
Hepatic Artery
1.Prompt systolic upstroke with acceleration time< 100 msec
2.Continuous flow throughout diastole
3.Resistive index between 0.5 and 0.7
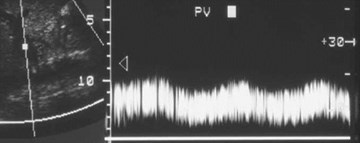
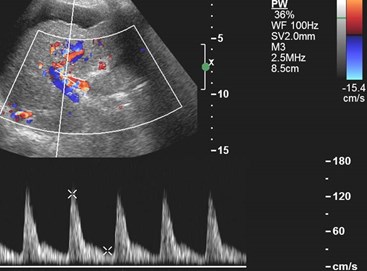
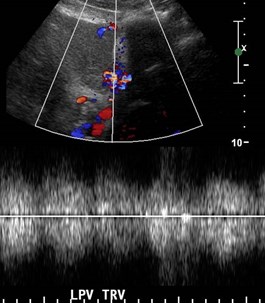
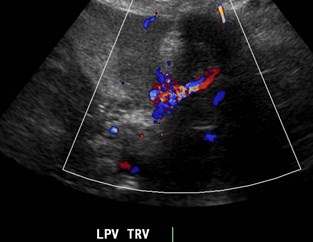
Portal Vein
1.Antegrade flow
2.Slight fluctuation due to respiratory variability
3.Maximum velocity range 13 – 30 cm/sec
4.Minimum velocity range 6 – 20 cm/sec
5.RI 0.39 0.1
Barakat BrJRad 2002;75:417
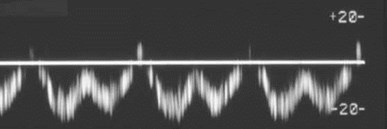
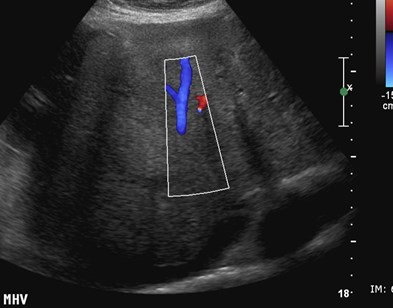
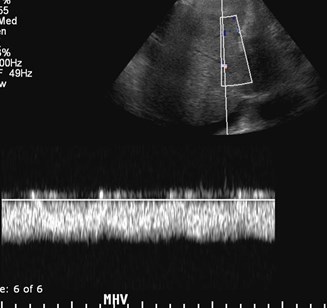
Hepatic Vein
1.Atrial and ventricular systole
2.Atrial and ventricular diastole
3.Deep inspiration increasesabdominal pressure reducingmesenteric blood flowing towardheart. This causes a dampening ofnormal phasicity.
Abu-Yousef JUM 1992;6:263
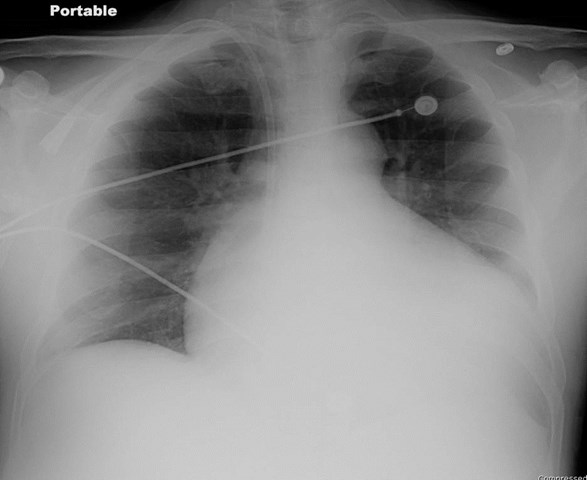
Elevated Right Heart Pressures
•Dilated hepatic veins
•Dilated inferior vena cava
•Hepatomegaly
•Ascites
•Accentuated hepatic venous pulsatility

Chronic Liver Disease
•Hepatic vein Doppler mirrors hemodynamics ofright atrium and reflect compliance of liver
•Abnormal Doppler consists of reduction inamplitude of phasic oscillation without reversedflow, eventually becoming completely flat
•Abnormal waveforms are typical of cirrhosis andmay also occur with fibrosis and/or steatosis,Budd-Chiari syndrome and diffuse metastases
•Hepatic vein waveforms can be used to monitorpatients response to vasoactive drugs for controlof variceal bleeding
Bolondi Radiology 1991;178:513
Colli AJR 1994;162:833
Baik Radiology 2006; 240:574
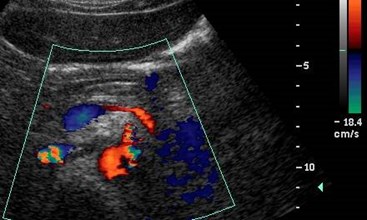
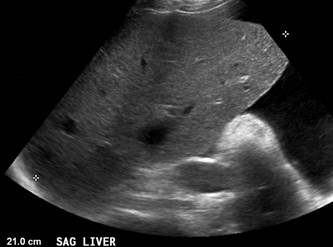
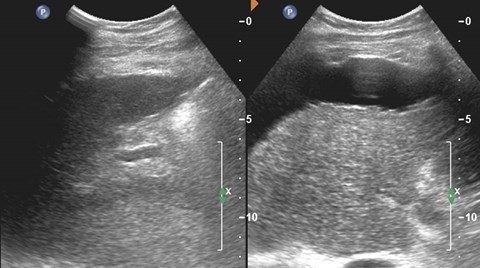
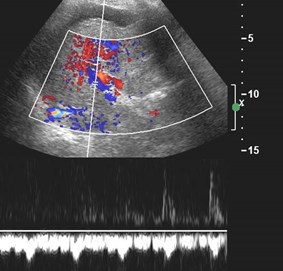
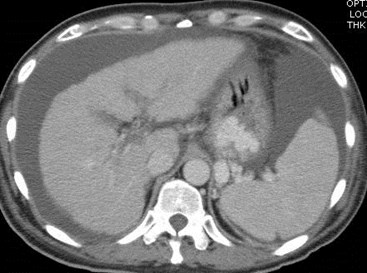
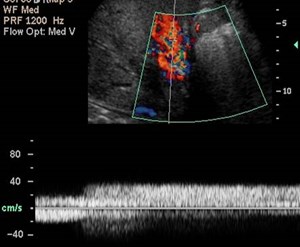
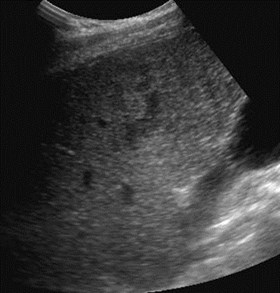
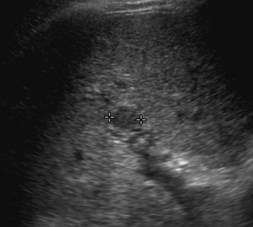
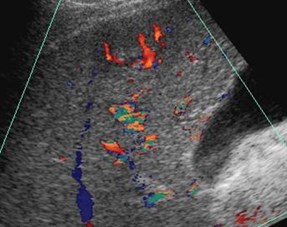
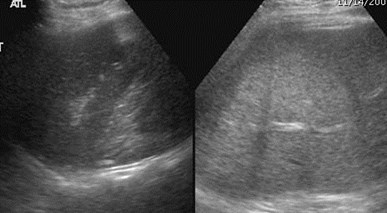
Nodular liver (regenerating nodules and fibrosis)indicating cirrhosis
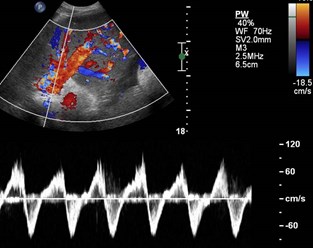
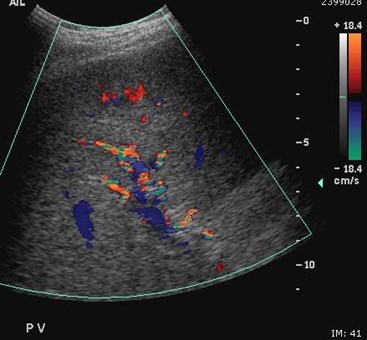
Biphasic portal vein flow
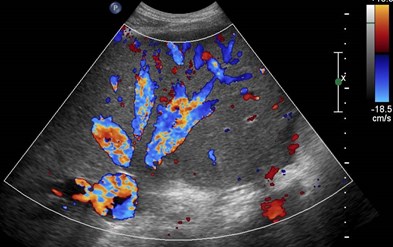
Exuberant arterial flow, high velocity, normal RI
Hepatofugal Flow in Cirrhosis
Spleen Liver



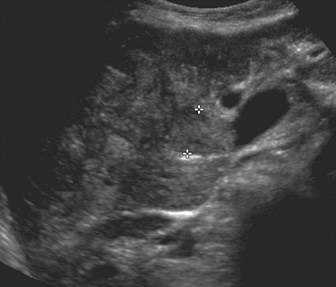
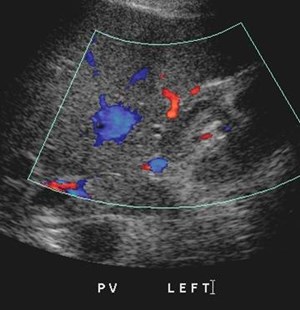
Portal Vein Thrombosis
•Associated with: malignancy, includingHCC, metastatic disease and pancreaticcarcinoma; chronic pancreatitis; chronichepatitis; septicemia; trauma;splenectomy; hypercoagulable states;acute dehydration
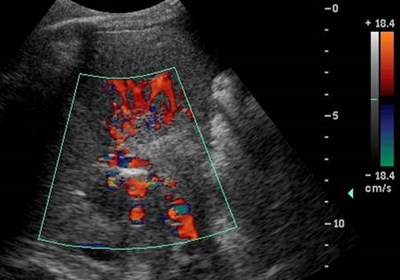


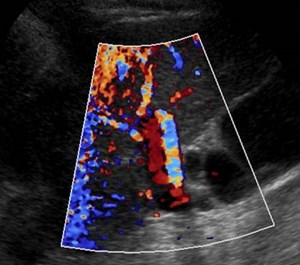
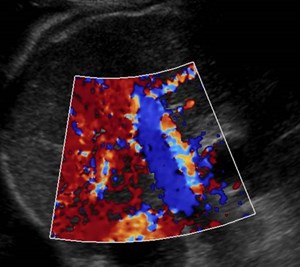
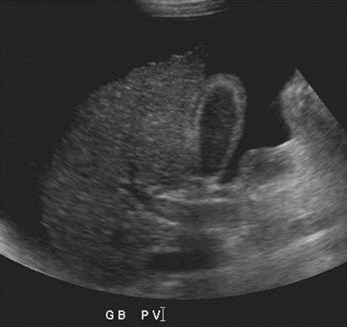
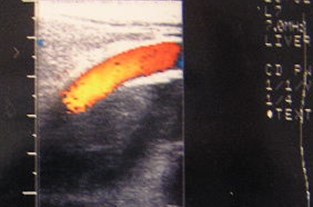
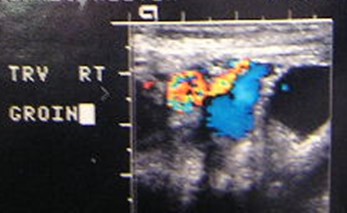
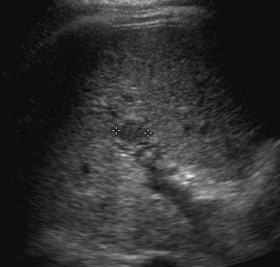
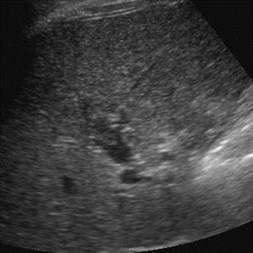
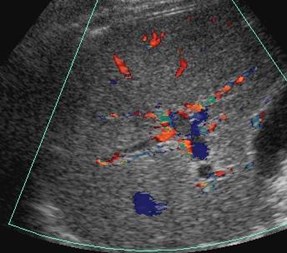
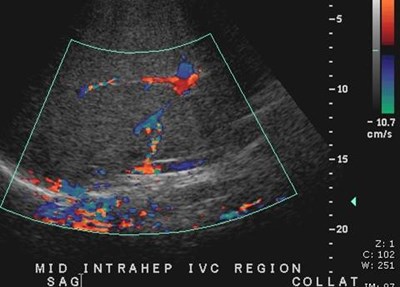
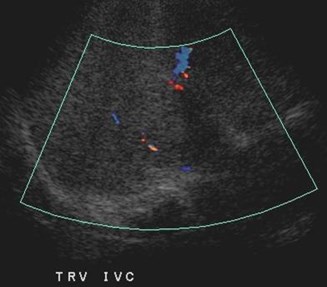
Cavernous Transformation of thePortal Vein
•Worm-like vessels at porta hepatis
•Represent peri-portal collateral circulation
•Results after long term portal veinthrombosis, requiring up to 12 months
•More likely to develop in benign disease
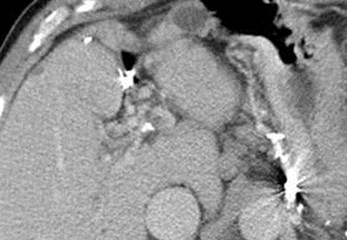


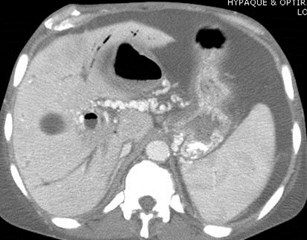
Chronic PVThrombosis withCavernousTransformation andcalcification of PV

Sag
Sag
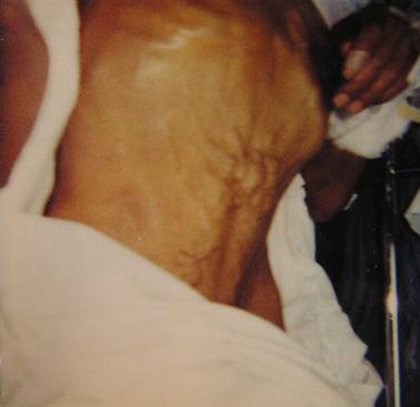
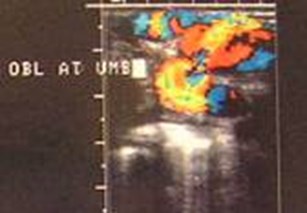
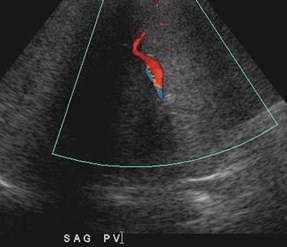
Para-umbilical vein varix andCaput Medusa
Dilated Paraumbilical Veins
•Small paraumbilical vessels may representvasa vasorum connecting veins aroundumbilicus to portal vein.
•Considered dilated if > 2mm
•Seen in 25 % patients with portal HTN
•Not a “recanalized” umbilical vein. Theumbilical vein never reopens afterobliteration
Merkle AJR 2005; 185:541

RPV




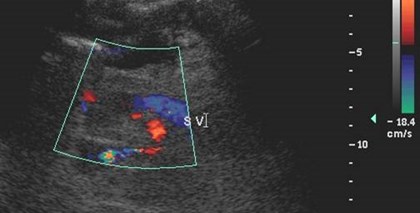
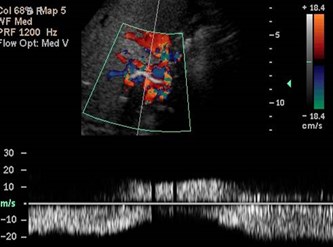
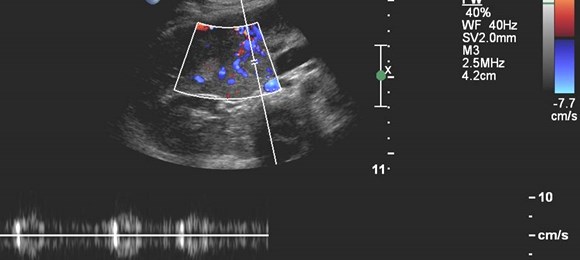
Malignant Portal Vein Thrombus
•Both bland and malignant thrombi maydemonstrate some continuous blood flow
•Pulsatile flow 95% specific for malignantthrombus
•Only 62% sensitive because manymalignant thrombi are hypo-vascular
Dodd AJR 1995;165:573
Hepatofugal PV flow and ?Two intra hepatic masses
Single peripheral HCC with localized PVTmistaken as a second lesion

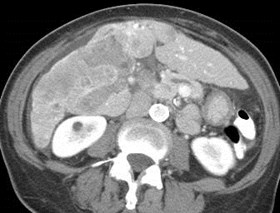
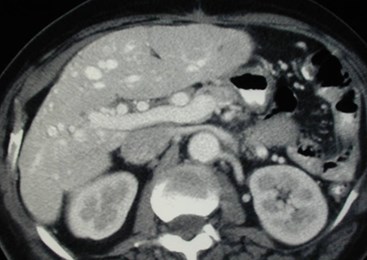
Transient Hepatic Arterial Difference(THAD) 2° localized PVT
Late arterial phase Late portal phase
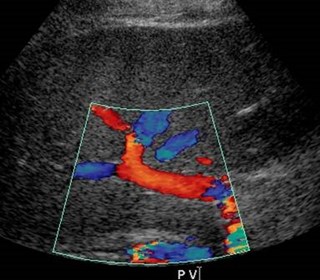
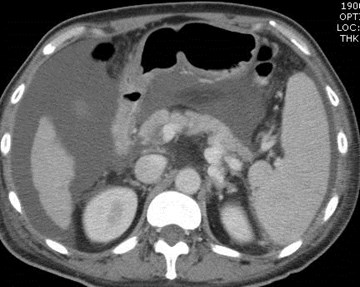
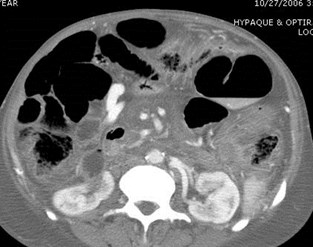
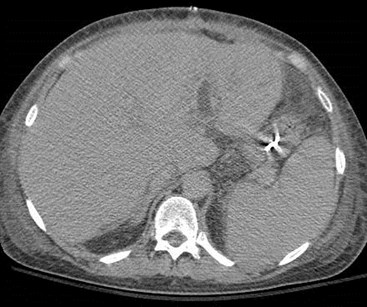
Normal main portal vein and thrombosis ofleft portal vein with normal appearance ofliver, much more difficult to appreciate onUS compared to CT
Liver Enhancement on CT
•At beginning of HAP (20-30 sec) liver enhancement isminimal. PV begins to enhance in later art phase, butcontrast has not yet filled sinusoids
•During PVP hepatic enhancement becomes maximal
•With vascular compromise, dual blood supply to liver cancause changes in volume and direction of blood flow onHAP with normal PVP
•Arterial and venous supply to liver are NOT independentbut have numerous communications (trans sinusoidal,vasal, tumoral, plexal routes)
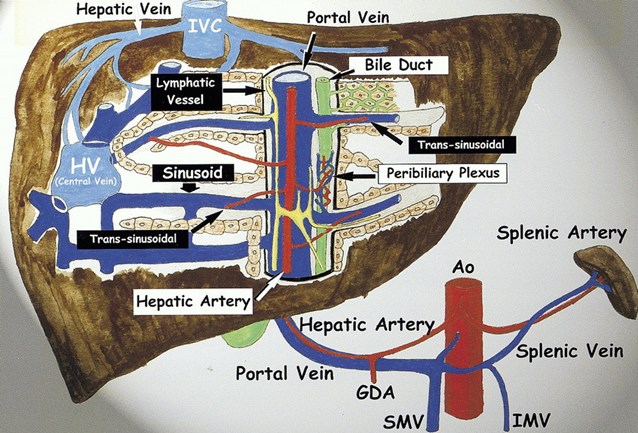
Quiroga, S. et al. Radiographics 2001;21:65-81
THAD or THPE
•Transient hepatic arterial difference
•Transient hepatic parenchymal enhancement
•Appears as high attenuation on HAP and normal on PVP
•Reflects enhanced, redistribution of arterial flow due todecreased portal or hepatic venous flow resulting inarterial-portal shunts
•May be lobar, segmental or subsegmental, usuallyperipheral and wedge shaped with straight margins andnormal vessels
•Causes include: PVT, cirrhosis, hepatic neoplasms,hepatic vein obstruction, aberrant blood supply,parenchymal compression, etc.
Quiroga, S. et al. Radiographics 2001;21:65-81


THAD due to atypicalhemangioma

Arterial-portal fistula
History of liver biopsy
34 yo, postpartum, elevated LFTs


Arterial Phase Portal Venous Phase
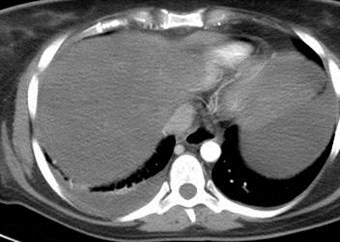
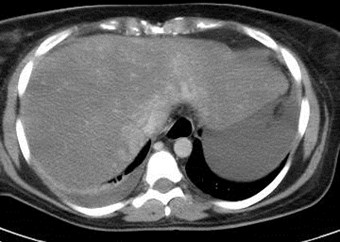
Budd-Chiari Syndrome



Man with paroxysmal nocturnal hemoglobinopathy
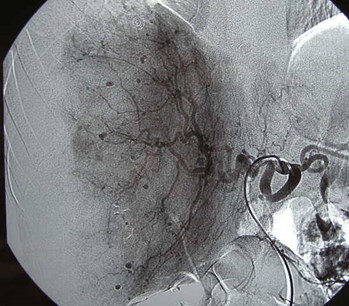
Budd-Chiari Syndrome
“spider web” pattern ofhepatic venous collaterals
Budd-Chiari Syndrome
•Occlusion hepatic veins
•Degree of occlusion and presence of collateralspredicts outcome. Some patients may die inacute phase of liver failure
•Causes: coagulation abnormalities such aspolycythemia rubra vera, chronic leukemia andparxysmal nocturnal hemoglobinuria; trauma,tumor extension from HCC, renal cell CA andadrenal CA; pregnancy; congenitalabnormalities; obstructing membranes, idopathic
•Clinical triad: ascites, hepatomegaly, abdominalpain
Murphy AJR 1986;147:9
Budd-Chiari Syndrome: US
•Hepatomegaly, ascites, hemorrhagic infarction
•Sparing of caudate lobe with hypertrophybecause of veins which drain directly into IVCbelow level of involved hepatic veins
• Partial or complete inability to visualize hepaticveins, extensive intrahepatic collaterals
•US may underestimate extent and presence ofthrombosis, especially with underlying cirrhosis
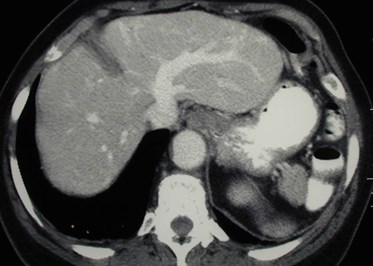
Budd-Chiari Syndrome: CT, MR
•HAP- normal or diffuse heterogeneity
•Initial PVP- prolonged heterogeneity, often withhomogeneous normal enhancement of caudatelobe
•Late imaging- caudate lobe de-enhances andrest of liver may become more homogeneous
•Poor visualization of hepatic veins
•Compression of IVC


Polyarteritis Nodosum
•A necrotizing vasculitis of small and mediumarteries (especially visceral) with microaneurysms
•Cause unknown, affects kidneys in 70 – 80%, GIinvolvement in 50%
•Must meet 3 of 10 criteria for diagnosis, of whichangiographic findings are one. Others include:weight loss, skin changes, testicular pain, diffusemyalgias, neuropathy, HTN, elevated BUN/creatinine, positive tissue biopsy
•Diff Dx: scleroderma, rheumatoid arthritis, SLE,Wegener’s granulomatosis, multiple drug abuse(metamphetamine)


Late arterial phase imaging
Osler-Weber-Rendu Disease
•Hereditary hemorrhagic telangiectasias
•Thin walled vascular channels with arterial tovenous connections
•Liver is a common organ of involvement thoughless frequentlly symptomatic
•In liver shunts occur between hepatic artery andportal and/or hepatic veins, resulting insimultaneous enhancement of these vessels.Hepatic arteries and veins will be dilated andtortuous with hepatomegaly
•Can lead to portal hypertension and cirrhosis


Two different patients
Focal Fat and Focal Sparing
•Characteristically occurs in specific areas:adjacent to falciform ligament or ligamentumvenosum, porta hepatis, gallbladder fossa
•Attributed to variant venous circulation such asanomalous gastric venous drainage
•Characteristics on imaging: location, fat density,geographic shapes, lack of mass effect
•Involved areas are usually small, butoccasionally can be larger and/or confluent,multiple small focal areas or perivascular indistribution
Hamer Radiographics 2006;26:1637